Clinical Dialogue Summarization
Libraries used: transformers, datasets, peft, evaluate, torch, pandas, numpy, matplotlib, sklearn, sentence_transformers
Concepts: EDA, fine-tuning Seq2Seq language model, LoRA, BERTScore, ROUGE, SentenceTransformer, t-SNE
Abstract
I’ve personally found text summarization to be one of the most useful applications of generative AI. If done well, auto-generated summaries save a lot of time and human effort and can increase understanding/reduce misunderstanding of the original text by picking out the key points and/or standardizing the summary format.
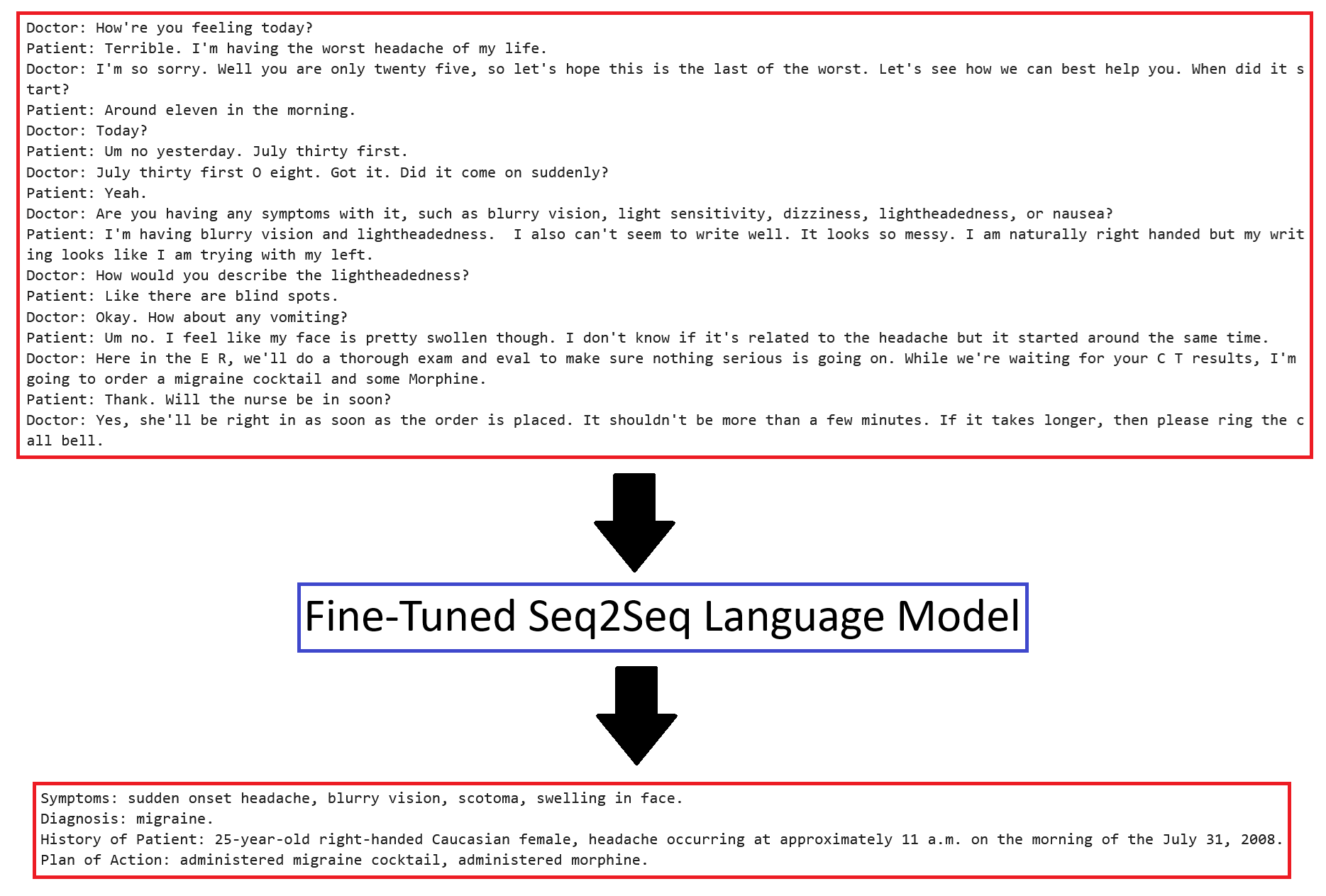
Text summarization can be applied to any field, but I chose to focus on a medical application. I found a dataset on Hugging Face consisting of 1301 samples of clinician-patient dialogue with summaries in bullet-point format (symptoms, patient history, diagnosis, plan of action). I fine-tuned BART-base on the dataset utilizing two strategies: (1) unfreezing the language modeling head and (2) applying LoRA. Training loss converges to nearly zero, with BERTScore and ROUGE approaching 1.0 for the entire training split, but validation performance only gets worse, even with dropout and weight decay. At this point, I suspected the problem was the dataset. I applied a SentenceTransformer to encode the dialogues and summaries and calculated the pairwise distances between samples. I chose one sample - the validation sample with the closest training sample match - to analyze. This sample talks about fractures and surgery. In the entire dataset, I found only 7 other samples related to fractures and surgery, and I found noisy samples with mismatched dialogues and summaries and samples with almost no information. The dataset is too small and noisy for the model to generalize. My next step is to explore augmenting the dataset with fake samples (e.g. generated by ChatGPT).
Project Summary
Ultimately, the fine-tuned model does not generalize because of the small and noisy dataset, which I explain below.
I found a dataset on Hugging Face that summarizes transcribed clinical dialogue. It’s a modified version of this dataset. The team that uploaded the modified dataset to Hugging Face added structure to the summaries, converting them from paragraph format to bullet-point format with 4 bullets: symptoms, diagnosis, patient history, and plan of action. The team only uploaded the training and validation splits.
The original dataset was intended for training both summarization and classification into medical categories, but for simplicity, I only attempted summarization.
The team that uploaded the dataset fine-tuned “facebook/bart-large-cnn”, but I chose to fine-tune “facebook/bart-base” for efficiency and because the dataset is very small – only 1301 samples.
These are my key discoveries from fine-tuning on this dataset:
- For accurate summaries, mean cross-entropy loss needs to be < 0.4. The model hallucinates at higher losses, which can drastically alter the meaning of the clinical note.
- With the language modeling head unfrozen or 38M trainable parameters, training loss is 0.07 after 15 epochs
- With all layers unfrozen or 140M trainable parameters, training loss is 0.07 after 15 epochs (almost no difference from unfreezing only the language modeling head)
- With the base model frozen and LoRA applied with rank=512 or 28M trainable parameters, training loss is 0.29 after 30 epochs
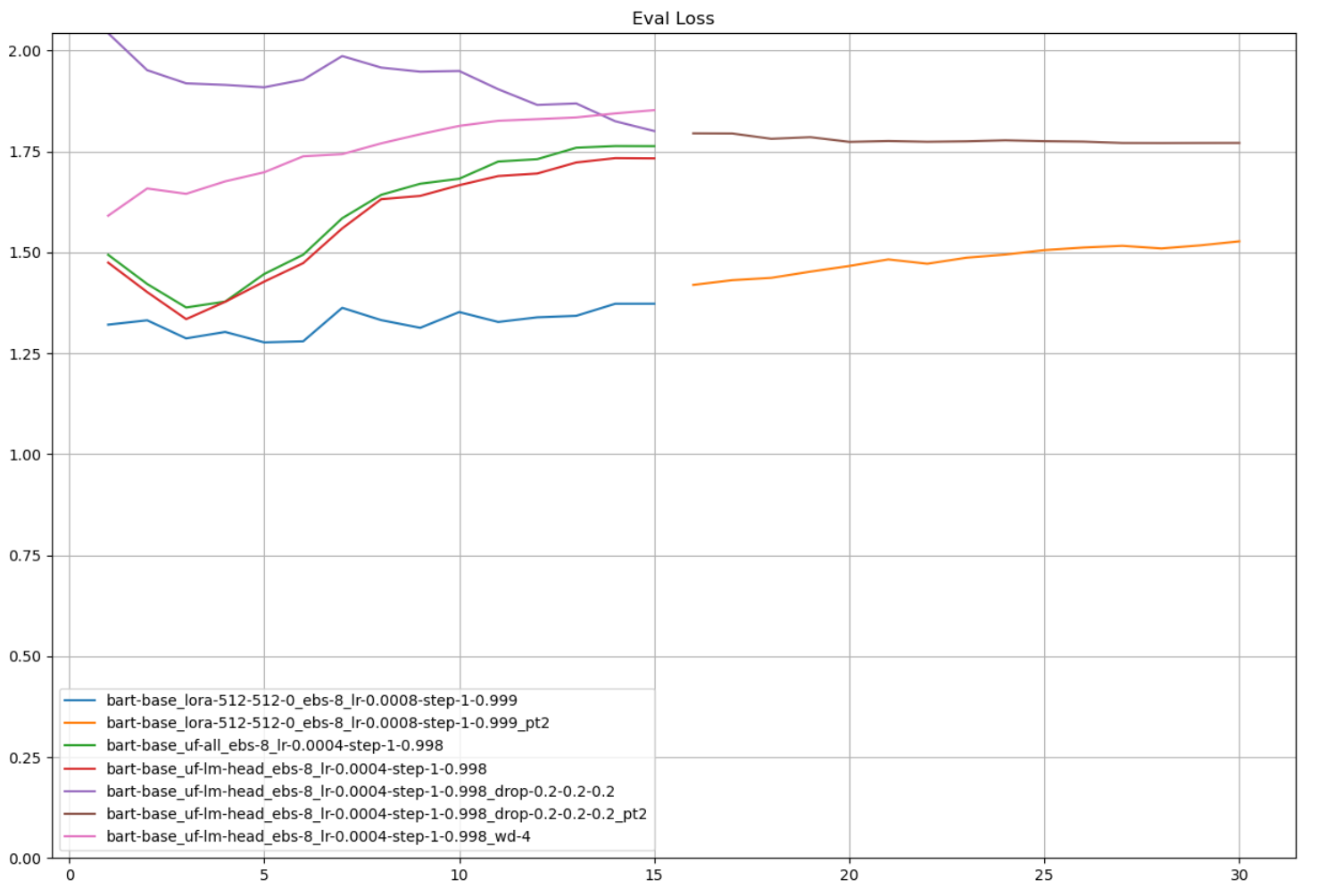
- In all cases, the model overfits. Validation loss increases as training progresses and never falls below 1. The dataset is too small and the task is too complex for the model to generalize – applying dropout and weight decay degrades both training and validation loss. The model generates summaries that are in the correct format and may even contain correct information, but the model often hallucinates, either contradicting the ground truth or contradicting itself.
- The dataset is too small and too noisy for the complexity of the task. For a given sample, there aren’t enough similar samples; some samples contain almost no information; and some samples have inaccurate ground truth summaries.
- Training across 5-fold training/validation splits are nearly identical, which means the problem isn’t splitting
- Encoding the dialogue and summary using a SentenceTransformer and then plotting the encodings using t-SNE shows that the dataset is quite scattered. I break down a specific example below.
- I generated summaries using dataset team’s model, and their model performs poorly
Training and Validation Loss
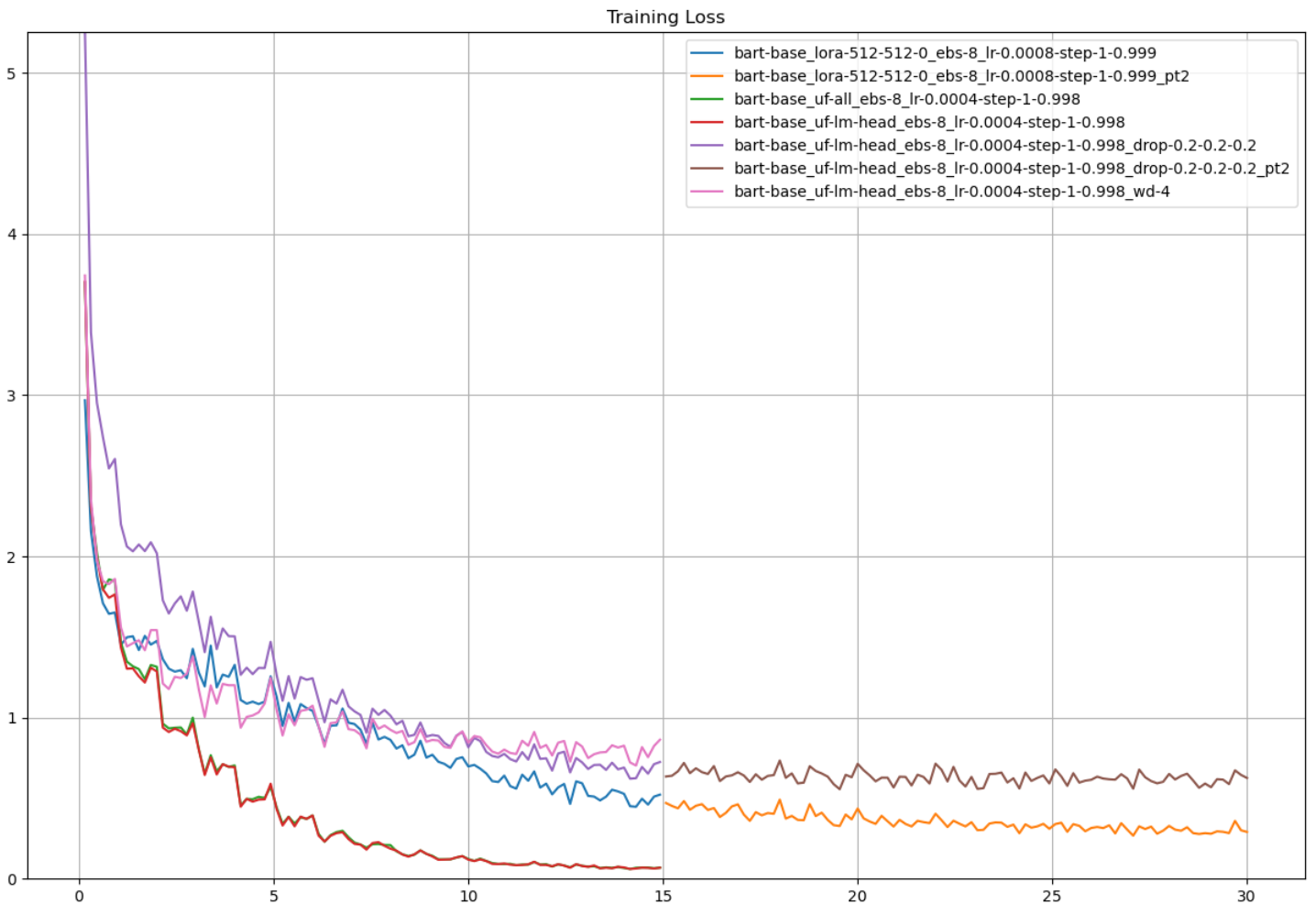
The plots below summarize the training results: I can achieve good training performance by either unfreezing layers in the base model or applying LoRA with a relatively high rank, but regularization degrades both training and validation performance.
Model configurations (top to bottom in the legend):
- LoRA (r = 512, alpha = 512, dropout = 0), effective batch size = 8, initial learning rate = 8e-4, StepLR(step_size = 1, gamma = 0.999)
- Continuation of training from #1
- Unfreeze all layers, effective batch size = 8, initial learning rate = 4e-4, StepLR(step_size = 1, gamma = 0.998)
- Unfreeze language modeling head, effective batch size = 8, initial learning rate = 4e-4, StepLR(step_size = 1, gamma = 0.998)
- Unfreeze language modeling head, effective batch size = 8, initial learning rate = 4e-4, StepLR(step_size = 1, gamma = 0.998), dropout = 0.2 (default 0.1)
- Continuation of training from #5
- Unfreeze language modeling head, effective batch size = 8, initial learning rate = 4e-4, StepLR(step_size = 1, gamma = 0.998), weight decay = 4 (default 0)
Compare 4-7, which all unfreeze the language modeling head. 4 (red) is with default dropout, 5-6 (purple-brown) is with all dropout rates set to 0.2, and 7 (pink) is with weight decay set to 4.
Dataset Visualization and Analysis
I investigated the dataset to try and find the reason why the model wasn’t generalizing.
- First, I trained on 5 train/val folds to rule out the train/val split. Training was nearly identical in all 5 runs.
- Second, I used a SentenceTransformer to encode the dialogues and summaries and then applied t-SNE to visualize the samples in 2D.
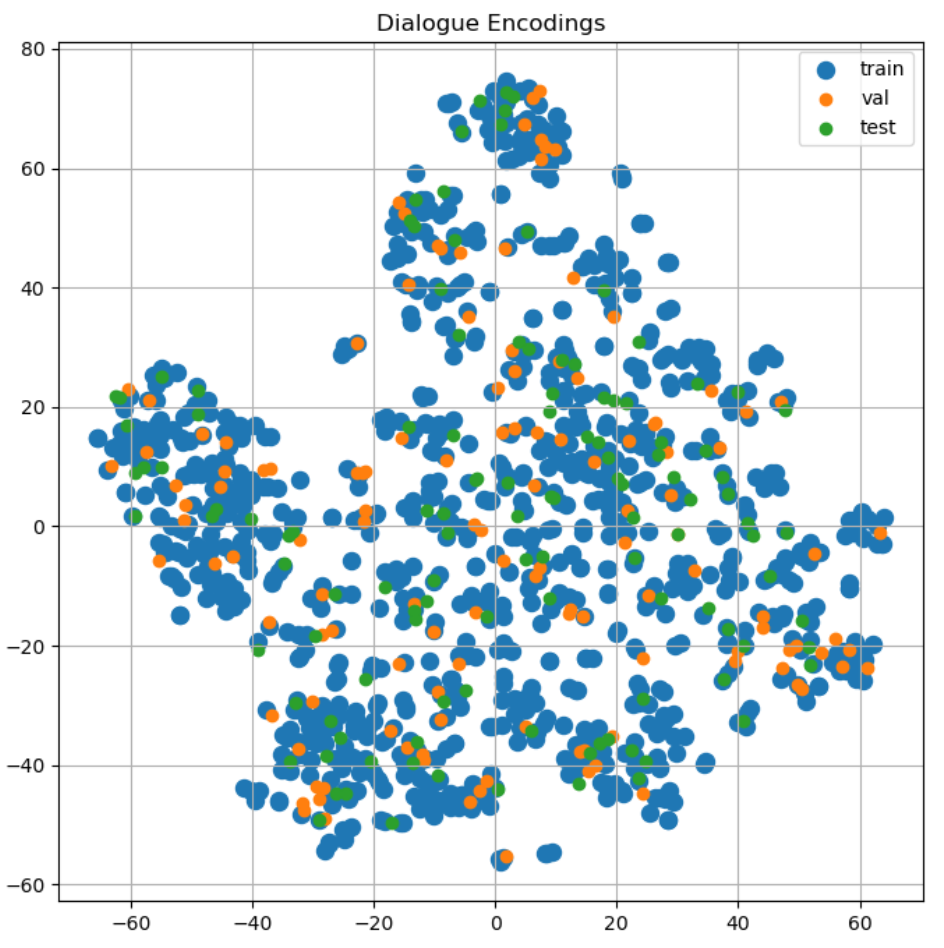
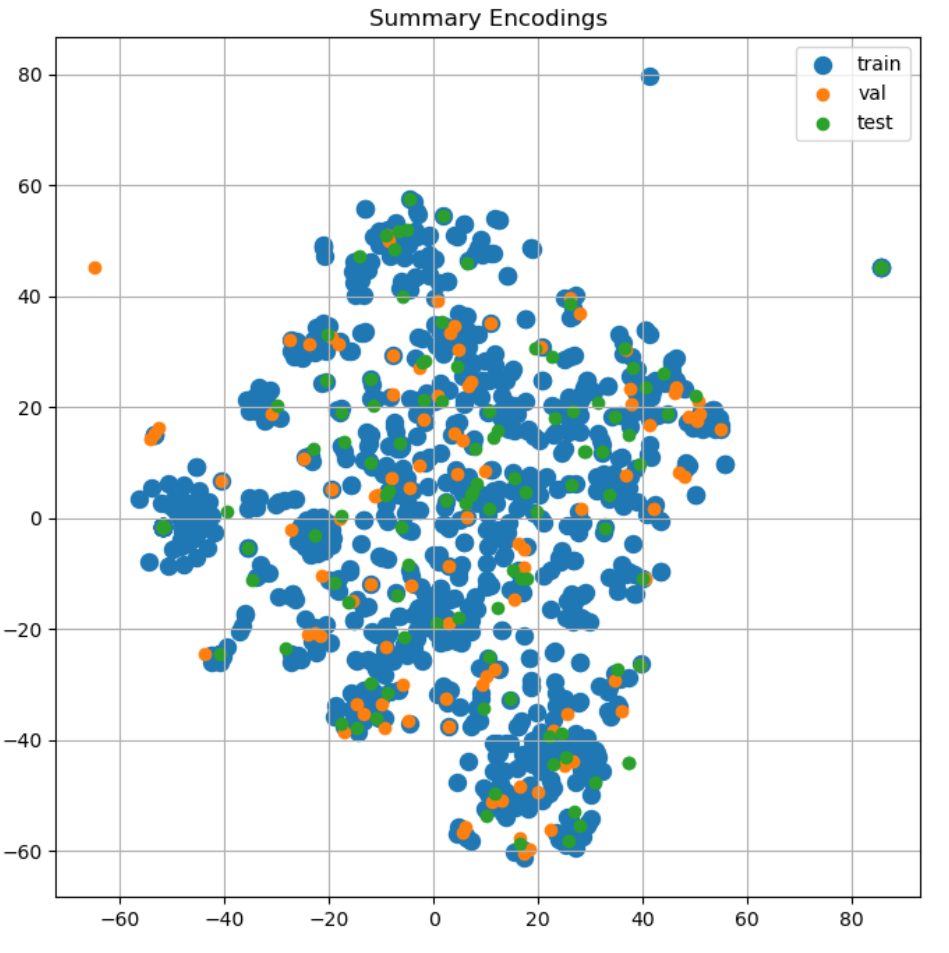
At first glance, the samples looked fine - nearly every validation and test sample is surrounded by training samples.
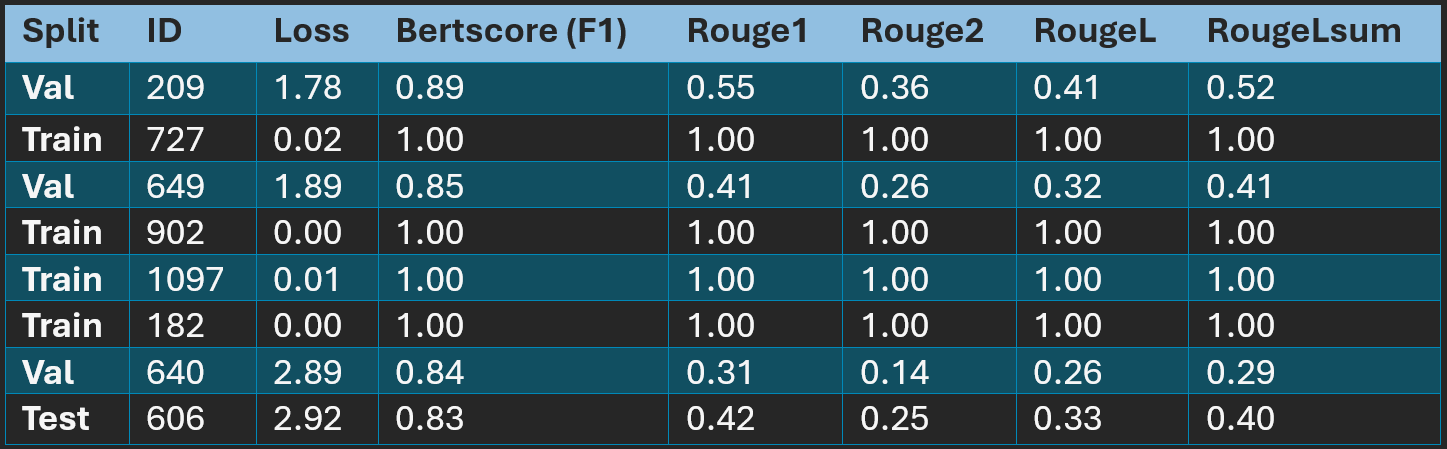
In the 2D space, by distance, validation sample ID 209 has the closest training sample match. For 209, I found the top 5 closest samples from training, validation, and test splits. Since 209 is about fractures and surgeries, I also searched the dialogues for any mention of fracture/fractures/fractured.
After reading through the sample texts, I identified only 8 samples related to fractures and surgery, which isn’t enough samples for a task of this complexity. I ran these samples through my model. The model generates perfectly matching summaries for the training samples but performs very poorly on the validation and test samples.
Hallucinations
It’s not just BERTScore and ROUGE - the model hallucinates. Take 209 for example:
Dialogue
Doctor: Good morning, young man. Are these your parents?
Patient: Yes.
Doctor: Good, can you tell me more about your son, please?
Guest_family_1: Well, he’s five now, and he fell onto his right arm on December fifth two thousand seven.
Doctor: After he fell, how was he treated?
Guest_family_1: We went to the E D right after he fell, and they said he had complete fractures of both bones in the arm.
Doctor: Yes, I see that here, he also has shortening bayonet apposition.
Guest_family_1: What can we do for this?
Doctor: There’s actually a few options here. First we can cast it and see how he heals, generally, children heal up very well from fractures.
Guest_family_1: That’s good, we like that option more than any kind of surgery.
Doctor: However, surgery is also an option here as well.
Guest_family_1: Yeah, to be completely sure we fix this, I think we should opt for the surgery, what do you think, honey?
Guest_family_2: Yes, I agree. What are the risks of infection for this surgery?
Doctor: The risk of infection is very low, generally less than one percent. We use antibiotics to control for infection.
Guest_family_1: Will he be asleep for the surgery?
Doctor: Absolutely, he won’t feel a thing. Other risks include bleeding, changes in sensation and motion of the extremity, hardware failure, and need for later hardware removal, and cast tightness. I would not worry about these risks. We have great results with these surgeries.
Guest_family_1: Then yes, we’d like to do the surgery.
Summary
Symptoms: refracture of right forearm
Diagnosis: complete fractures of both bones in right arm, shortening bayonet apposition
History of Patient: fell onto right arm on December 5, 2007
Plan of Action: surgery for closed reduction and pinning, with risks including anesthesia, infection, bleeding, changes in sensation and motion of extremity, hardware failure, need for later hardware removal, cast tightness
Prediction
Symptoms: fell onto right arm on December 5, 2007, incomplete fractures of both bones in right arm, shortening bayonet apposition, possible need for later hardware removal and possible continuous nerve Symptoms
Diagnosis: N/A
History of Patient: fell onto right arm on December 5, 2007, incomplete fractures of both bones, received physical therapy and bandaging, no other surgeries recommended due to risk of infection
Plan of Action: Surgery recommended due to non-healing extremity injuries, risks of infection discussed and patient agreed to surgery after informed consent
Analysis: The model is hallucinating – it thinks the fractures are incomplete fractures and contradicts itself by saying that surgery is both recommended and not recommended due to risk of infection.
The ground truth summary contains information not present in the dialogue (noisy dataset).
Noisy Samples and Samples Without Information
While investigating the dataset, I found noisy samples and samples without information.
For example, the dialogue in training sample ID 931 is about a fracture, but the summary is about heart problems.
Doctor: Hello. How are you all doing today?
Guest_family: We’re doing fine. I’m the mother of my four year old boy.
Doctor: Hello, ma’am. What seems to be the problem?
Gest_family: We just wanted to follow up after my son’s E R visit.
Doctor: Oh, no. What happened?
Guest_family: He was playing at the park and thought it was a good idea to jump off the swing. Crazy kid, right?
Doctor: It happens. Live and you learn, as they say. Do you have any information from the E R visit.
Guest_family: I gave it to the nurse. Did you not get it?
Guest_clinician: Sorry. I got really busy, but here is the report.
Doctor: Could you read it to me, please?
Guest_clinician: Of course. So, their son severely injured his left distal humerus. No problems were claimed before the injury. The E R saw him for his deformed elbow.
Doctor: Are there any exams on the report?
Guest_clinician: There is an x ray and physical exam. They both confirmed a closed type three supracondylar fracture of his left distal humerus with severe puckering of the skin anteriorly with major ecchymosis in the same region. He did have a radial pulse palpable
Doctor: Thank you, nurse. Mom, were you there before his surgery?
Guest_family: My husband and I were. My husband rushed from this cultural event he had planned.
Doctor: I see. What do you all identify as?
Guest_family: We identify as white.
Doctor: I see. I’m going to perform a neurological exam on your son now. Hi buddy. Is it fine if I do a quick exam?
Patient: Sure.
Doctor: Thanks. It’ll be quick.
Patient: Okay.
Doctor: After doing the exam I see his ulnar, median, and radial nerves are intact. I couldn’t do the entire exam because the pain might be too much for him.
Guest_family: Thank you so much for your help.
Symptoms: N/A
Diagnosis: N/A
History of Patient: patient had cardioversion for atrial fibrillation, taking Coumadin, history of smoking but quit several years ago, denies COPD or emphysema, no family members are sick
Plan of Action: N/A
Training sample ID 219 contains almost no information.
Doctor: So, I am looking at his x ray and it does not show any open fracture or any kind of bone abnormality.
Guest_family: Okay, I was really worried about my son.
Doctor: I understand, but like I said, I didn’t see any open fracture in his x ray report nor any abnormality.
Guest_family: Okay.
Symptoms: N/A
Diagnosis: N/A
History of Patient: N/A
Plan of Action: N/A
.